2024: Volume 6, Issue 1
Past Issues
 Abstract
Abstract  PDF
PDFDental Caries Experience of Primary School Children
Abdalmawla Alhussin Ali1,*, Karima Ali Belgasem2
1Department of Orthodontics, Faculty of Dentistry, Sirte University, Libya
2Department of Oral Pathology, Faculty of Dentistry, Sirte University, Libya
*Corresponding Author: Abdalmawla Alhussin Ali, Professor (Assistant) in Orthodontics Department of Orthodontics, Faculty of Dentistry, Sirte University, Libya; Tel: 00218-91-0544754; Email: [email protected]
Received Date : April 5, 2024
Publication Date: April 17, 2024
Citation: Ali AAA. (2024). Dental Caries Experience of Primary School Children. Dental. 6(1):12.
Citation: Ali AAA. © (2024).
ABSTRACT
Dental caries among children is common but there is scarcity of updated data about its prevalence among children. The aim of this study was to assessment of the caries experience of primary school children in Sirte – Libya. Materials and methods: A descriptive cross-sectional study, the total eligible sample comprised 521 students, 373 of them females and 248 males, aged between 5 and 13 years. Participants were examined for dental caries, using the decayed, missing and filled teeth index (DMFT/dmft) according to the WHO criteria, which were done by three dentists with dental mirror, dental explorer and ordinary room light. Results: Among 119 children aged 5-7 years, 74.0% had decay in their teeth, with a mean DMFT/dmft of 3.5± 3.1. Among 156 children aged 8-10 years, 84.0% had dental caries, with a mean DMFT/dmft of 3.3± 2.9. While, in the 11-13 years group, 69.1% had caries lesions with a mean DMFT/dmft of 2.8±2.6. Conclusions: Dental caries prevalence and severity in 5 and 13year-olds primary school students in Sirte were high, there is an urgent need for oral health programs targeted at the treatment and prevention of dental caries in these children.
Keywords: Dental caries, prevalence, children, DMFT/dmft index, Sirte- Libya
INTRODUCTION
Dental caries is the most common preventable childhood diseases it is the primary cause of oral pain and tooth loss. The World Health Organization (WHO) reports that 60–90% of children are affected by dental caries [1]. It is affects both genders, all age groups all socioeconomic state and all races. It can be arrested and potentially reversed in its early stages, but is often not self-limiting and without proper care, caries can progress until the tooth is destroyed [2,3].
Dental caries is a multifactorial disease that starts with microbiological shifts within the complex biofilm and is affected by consumption of dietary sugars, exposure to fluoride salivary flow and composition and by cleaning teeth). Previous review of caries in young children worldwide which reported that studies from majority of the developing countries report a caries prevalence of higher than 50%. Reasons proffered for this disparity include changes in dietary habits and inadequate exposure to fluorides in developing countries [4].
Dental caries significantly impacts child health, If not treated [5,6]. Maintaining oral health at the individual level would lead to a shift in dentistry practice from restorative to preventive-oriented strategies, by reducing sugar intake, exposure for fluoride and proper use of fissure sealants. Availability of good data about the prevalence and distribution of dental caries is necessary dental preventive and therapeutic services [7].
Due to the poor health system and political instability that has its impact on the health of people, previous studies reported, the prevalence of dental caries in Libya showed an upward trend [8-10]. Furthermore, carious status of Libyan population is not regularly assessed; therefore, it is difficult to plan effective preventive interventions in the country (9). There are fewer childhood caries studies in Sirte –Libya. The objective of the present study was to determine the prevalence, severity and pattern of caries in primary school children in Sirte –Libya.
PATIENTS AND METHODS
This descriptive cross-sectional study, was carried out over 6 months starting from February to July 2022. The study was conducted on 521 of school children attending public primary schools for boys and girls in Sirte city. The sample had 273 girls and 248 boys. Four public primary schools were randomly selected to be included in this study, Formal consent was obtained from mangers of the involved schools.
The clinical examinations of all participants were carried out within their schools by three examiners were trained within faculty of dentistry of Sirte University. The examinations include taking data from students (Name, age and sex) and behavioral data on dietary. Students were examined for dental caries, using the decayed, missing and filled teeth (DMFT/dmft) according to the WHO Oral Health Survey Basic Methods [11]. A disposable diagnostic kit was used for each child in order to reduce the risk of cross infection, as well the examiner used disposable gloves and masks. Each subject was examined while seated on a portable chair and the examination was done under ordinary room light using a plane mouth mirror, an explorer, gauze, disposable gloves and masks to reduce the risk of infection. No radiographs were taken. The findings of the DMFT/dmft index, in addition to the demographic information's were recorded in a specially prepared form.
Data analysis was carried out using the Statistical Package for the Social Sciences (SPSS version 20 Inc. Chicago IL, USA) and Microsoft Excel. The statistical data were calculated included: mean, standard deviations and P value. P value was calculated significant at < 0.05.
RESULTS
The total number of children approached for this study was 521 25.. Out of 521 children examined, 273 (52.4%) were female and 248 (47.6%) were male (Figure 1). Their ages ranged from 5-13 years, and the mean age for all sample were 9.1 ± 2.8 years. The children were divided into three groups according to age. With 119 students (22.8%) aged 5-7 years, 156 individuals (29.9%) aged 8-10 years and 246 ones ( 47.2%) aged 11-13 years, (Table 1) summarizes the age and gender characterization of the sample.
Figure 1: Distribution according to gender.
Table 1: Age and gender characterization of the sample.
|
Variable N=521 (%) |
||
|
Gender |
Male Female |
248 (47.6%) 273 (52.4%) |
|
Age |
5-7 8-10 11-13 |
119 (22.8%) 156 (29.9%) 246 (47.2%) |
The total percentage of primary schoolchildren who experienced caries was 74.7%, while the percentage of those who are free of caries was 25.3% (Figure 2).
Figure 2: Prevalence of dental caries among primary schoolchildren.
Prevalence of Dental Caries According to Age
Regarding the 5-7 years age group, 31 (26.0%) students were found to be caries free teeth, while 88 children (74.0%) had dental decay dental caries in one tooth or more, with a mean dmft of 3.5± 3.1. The major constituent of the dmft score was the decay (d) component (91.1%), (5.9%) missing teeth due to decay and small percentages had fillings (3.0%). In the 8-10 years age group, 131 (84.0%) of participated had one or more caries lesion and the number of caries free participants was 25 (16.0 %), As for the (D/d) component, it was found that (71.5%) of children who have had one decayed tooth or more (15.2%) had filling teeth had filling teeth and (13.3%) missing teeth due to dental caries. The mean with a mean DMFT/dmft of 3.3± 2.9. Concerning the 11-13 years age group, 170 (69.1%) children had dental decay in their permanent teeth, 76 (30.9%) students were found to be caries free teeth with a mean DMFT of 2.8± 2.6. Most of the students with untreated dental caries (decay) teeth (71.8%), (14.8%) of the sample in this group had filling teeth and (13.4%) of sample had missing teeth due to caries lesions (Figure 3). Regarding to age, there was no significant difference between the age groups in our study (Table 2).
Table 2: DMFT/dmft index evaluation for all age groups.
|
|
Variable |
5-7ys N % |
8-10ys N % |
11-13ys N % |
|
Decayed Teeth |
D/d ≥ 1 |
80(91.1%) |
93(71.5%) |
122(71.8%) |
|
Missed Teeth |
M/m ≥1 |
44(5.9%) |
17(13.3%) |
23(13.4%) |
|
Filled Teeth |
F/f ≥ 1 |
26(3.0%) |
20(15.2%) |
25(14.8%) |
|
|
|
3.5± 3.1 |
3.3± 2.9 |
2.8± 2.6 |
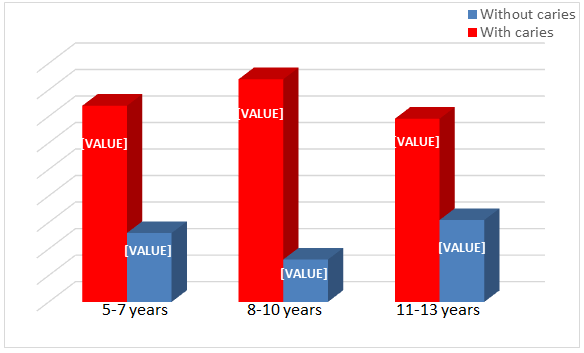
Figure 3: Prevalence of dental caries according to age.
Prevalence of Dental Caries According to Gender
Out of 521 students examined in this study, 273 (52.4%) were females and 248(47.6%) were males. The prevalence of dental caries among females was found to be (54.0%) with the mean DMFT/dmft score of 4.81 ± 4.53. (46.0%) of males were affected by dental caries with the mean DMFT/dmft for males was 4.28 ± 3.72. Even though the prevalence of dental caries and the mean of DMFT/dmft scores were slightly high among the females, the difference was not statistically significant (Table 3).
Table 3: Caries experience of primary school children by gender
|
|
Female (54.0%) Mean ± SD |
Male (46.0%) Mean ± SD |
P-value
|
|
D (d) |
3.63 ± 2.31 |
3.42 ± 2.30 |
NS |
|
M(m) |
1.15 ± 2.05 |
1.01 ± 2.0 |
NS |
|
F(f) |
0.764 ± 2.681 |
0.31 ± 1.02 |
NS |
|
DMF/dmf |
4.81 ± 4.53 |
4.28 ± 3.72 |
NS |
NS: None statically significant
DISCUSSION
Dental caries has long been a global oral health burden. It is affects all age groups, although children are affected to a greater extent. The aim of this study was to assess prevalence of caries among children aged 5–13 years. The results of this study indicated that the caries prevalence and severity among students of primary school in Sirte –Libya was high and, the total caries prevalence of 74.7% among school children. Decay component was the major component in the DMFT/dmft score, this indicates a very high percentage of untreated caries.
In our study the prevalence of dental caries among children aged 5-7 years was high the mean dmft of 3.5± 3.1, this result was consistent with the findings of Kumar et al. [12], which reported that 78.6% of school aged children in Sebha city –Libya had dental caries. Also this result match that in earlier study which indicated 78.0% among first-grade children in Tripoli –Libya [13], however, the caries prevalence among these group children in our study was substantially higher than the prevalence previously reported from other cities of Libya. 55% and 63.5 of children aged 6 years in Zawia and Zehra [14] and in Benghazi respectively [15] had caries lesions in their teeth.
The total caries prevalence of 84.0% among 8-10 years children in our sample had dental caries in their teeth, this findings match that reported in previous study in Sebha [12] and Benghazi [8]. This result is considered higher than the prevalence of DC in Tripoli city in 2021, at which the prevalence of caries was 48.2% [13]. The higher caries severity and prevalence in children could possibly be attributed to lower exposure of these children to preventive dental health education. The present cross sectional study was conducted in primary school children of 11-13 years found the prevalence of dental caries was 69.1%, this percentage is considered higher than that found in other Libyan cities: 57.8% and 32.7% in Benghazi and in Tripoli respectively [8,16].
In our study, the prevalence rate of DC found was 54.0% in females, whereas it was 46.0 % in males. Similar result that reported in previous studies from Tripoli-Libya found that the prevalence of DC is more in female than in male and the authors attributed that to eruption of teeth in females is earlier than in males or females eat more sugary food [17,18], the similar finding was found in other previous study [19-21]. Another study done in India have converse findings, which founded that caries prevalence is higher in males more than females and the authors attributed that to that males eat more than females in Indian society [22,23].
CONCLUSION
The present study has provided important information about dental caries status of primary school children in Sirt- Libya and useful baseline data for future comparisons. Furthermore, the caries prevalence and severity information would assist in the determination of treatment needs and preventive efforts required for those group of people.
REFERENCES
- Oral Health. (2018). Geneva: World Health Organization.
- Denloye O, Ajayi D, Bankole O. (2005). A study of dental caries prevalence in 12‑14 years old school children in Ibadan, Nigeria. J Paediatr Dent. 15:147‑151.
- Al-Samadani H, Ahmad S, Bakeer A, Elanbya G. (2017). Oral health knowledge and practice among 9-12-year-old schoolchildren in the region of Madinah, Saudi Arabia, and its impact on the prevalence of dental caries. Eur J Gen Dent. 6:54-58.
- Stephen W. (1994). Caries in young populations-Worldwide. In: Cariology for Nineties. Bowen W H,Tabak LA. Eds. Rochester: University of Rochester Press.
- Petersen E. (2003). The World Oral Health Report 2003: continuous improvement of oral health in the 21st century--the approach of the WHO global Oral health Programme. Community Dent Oral Epidemiol. 31:3-23.
- Krisdapong S, Prasertsom P, Rattanarangsima K, Sheiham A. (2013). School absence due to toothache associated with sociodemographic factors, dental caries status, and oral health‐related quality of life in 12‐ and 15‐year‐old Thai children. J Public Health Dent. 73:321-328.
- Irish Oral Health Services Guideline Initiative. (2009). Strategies to prevent dental caries in children and adolescents: evidence-based guidance on identifying high caries risk children and developing preventive strategies for high caries risk children in Ireland. Cork: Oral Health Services Research Centre.
- Huew R, Waterhouse P, Moynihan P, Maguire A. (2011). Prevalence and severity of dental caries in Libyan schoolchildren. Int Dent J. 61:217-223.
- Peeran SW, Altaher OB, Peeran SA, Alsaid FM, Mugrabi MH, Ahmed AM, et al. (2014). Oral health in Libya: addressing the future challenges. Libyan J Med. 9:23564.
- Sullivan R, McQuinn B, Purushotham A. (2011). How are we going to rebuild public health in Libya? J R Soc Med. 104:490-492.
- WHO. (2013). Oral health surveys: basic methods. 5th ed, Geneva: World Health Organization.
- Kumar P, Peeran S, Abdalla K, Al-Zain M. (2013). Dental caries status among 6–14 years old school going children of Sebha city, Libya. J Indian Assoc Public Health Dent. 11:18–22.
- Hosam A, Ahmid E, Reema B. (2021). Prevalence of dental caries and associated factors among school‑aged children in Tripoli,Libya: a cross‑sectional study.Alraqiq et al. BMC Oral Health. 21:224.
- Nasr AM, Moheb DM, Elmasry ES. (2014). Prevalence of dental caries in child school from two Libya’s western cities with fluoride in their drinking water. J Nat Sci. 12:28–34.
- Hawew RM, Ellwood RP, Hawley GM, Worthington HV, Blinkhorn AS. (1996). Dental caries in children from two Libyan cities with different levels of fluoride in their drinking water. Community Dent Health. 13(3):175-177.
- Kabar A, Elzahaf R, Shakhatreh F. (2019). Prevalence and Risk Factors of Dental Caries Among 6 To 12 Years Old Children In Tripoli City, Libya. Sch Dent Sci. 6:23-233.
- Armfield J, Mejıa G, Jamieson L. (2013). Socioeconomic and psychosocial correlates of oral health. Int Dental J. 63:202-209.
- Baccush M, Nayak C. (1991). Prevalence of dental caries in schoolchildren from a suburban area in Tripoli, Libya. Acta Stomatologica Croatica. 25:5-11.
- Gandeh M, Milaat W. (2000). Dental caries among schoolchildren: report of a health education campaign in Jeddah, Saudi Arabia (1996-97). Eastern Mediterranean Health Journal. 6: 396-401.
- Ali AA, Belgasem KA. (2023). Dental Caries Experience of Children with Autism Spectrum Disorder. Acta Scientific Dental Sci. 7(2).
- Ding L. (2015). Prevalence of permanent teeth caries among primary and secondary school students in Suzhou in 2015. Chinese J Child Health Care. 25:621-624.
- Ali AA, Belgasem KA. (2023). Oral Hygiene Status of Children with Autism Spectrum Disorders: Cross Section Study. Mathews J Dent. 7(1):1-3.
- Prabakar J, Arumugham I, Sri Sakthi D, Kumar R, Leelavathi L. (2020 ). Prevalence and Comparison of Dental Caries experience among 5 to 12 year old school children of Chandigarh using dft/ DMFT and SiC Index: A Cross-sectional study. J Family Med Prim Care. 9:819-825.